
Neurology:尿储留诱发的可逆性脑血管收缩综合征
2022-02-16 “脑血管病及重症文献导读”公众号 “脑血管病及重症文献导读”公众号

突发2次为期30min的霹雳样头痛、视力丧失、新发尿失禁、高血压(200s/90s[译者注:这是什么单位?)和心动过缓超过24小时。
18岁,男性。
创伤事故后C6以下四肢瘫。
突发2次为期30min的霹雳样头痛、视力丧失、新发尿失禁、高血压(200s/90s[译者注:这是什么单位)和心动过缓超过24小时。
影像学显示多发脑血管狭窄(图1)、弥散抑制和T2/FLAIR高信号(图2);经颅多普勒(TCD)显示血流速度增加。诊断为可逆性脑血管收缩综合征(RCVS)。
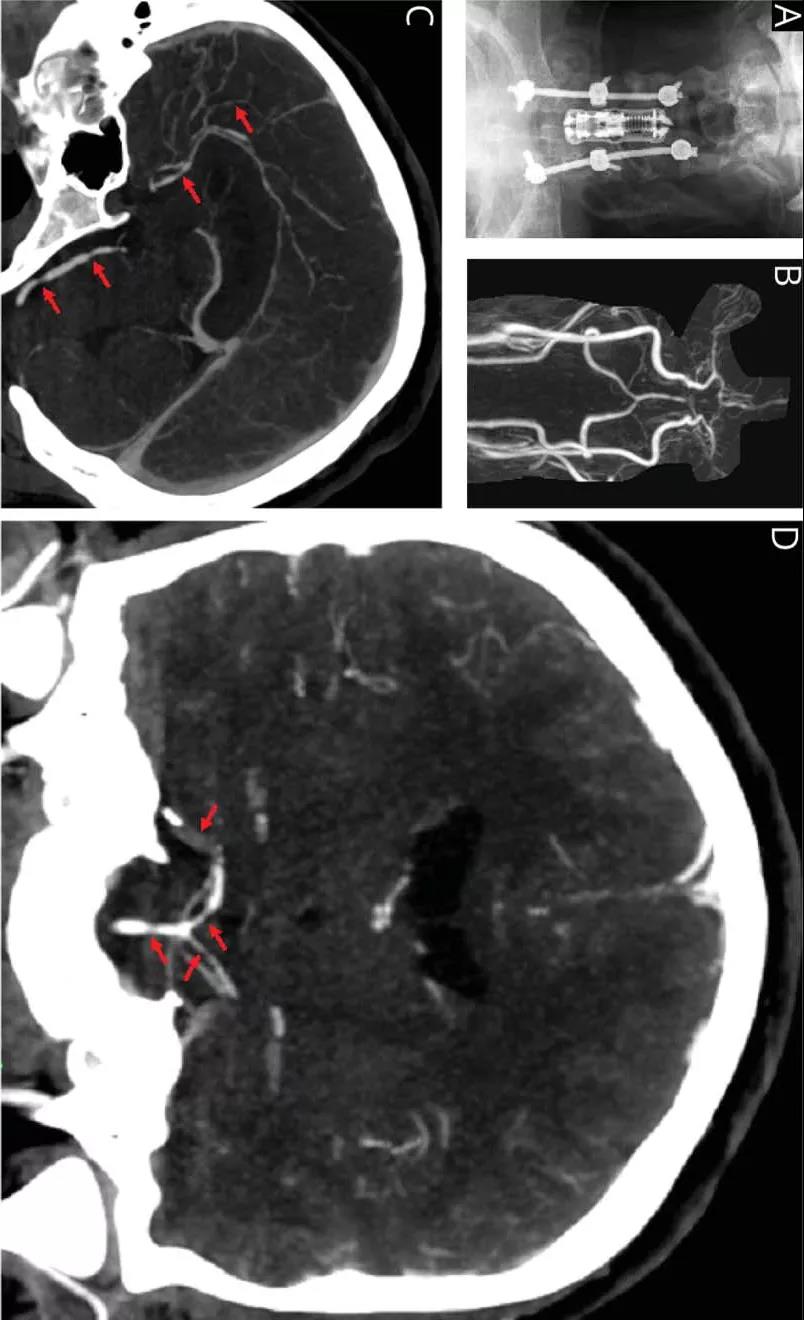
下图1.(A)外伤事故后置入的脊柱硬件(Spinal hardware)。从C4到C7颈椎前路脊柱融合,以及从C4到上胸椎后路脊柱融合。(B–D)急性头痛和视力丧失临床恶化时完成的CTA。箭头显示了后部和前部血管的弥漫性血管痉挛:
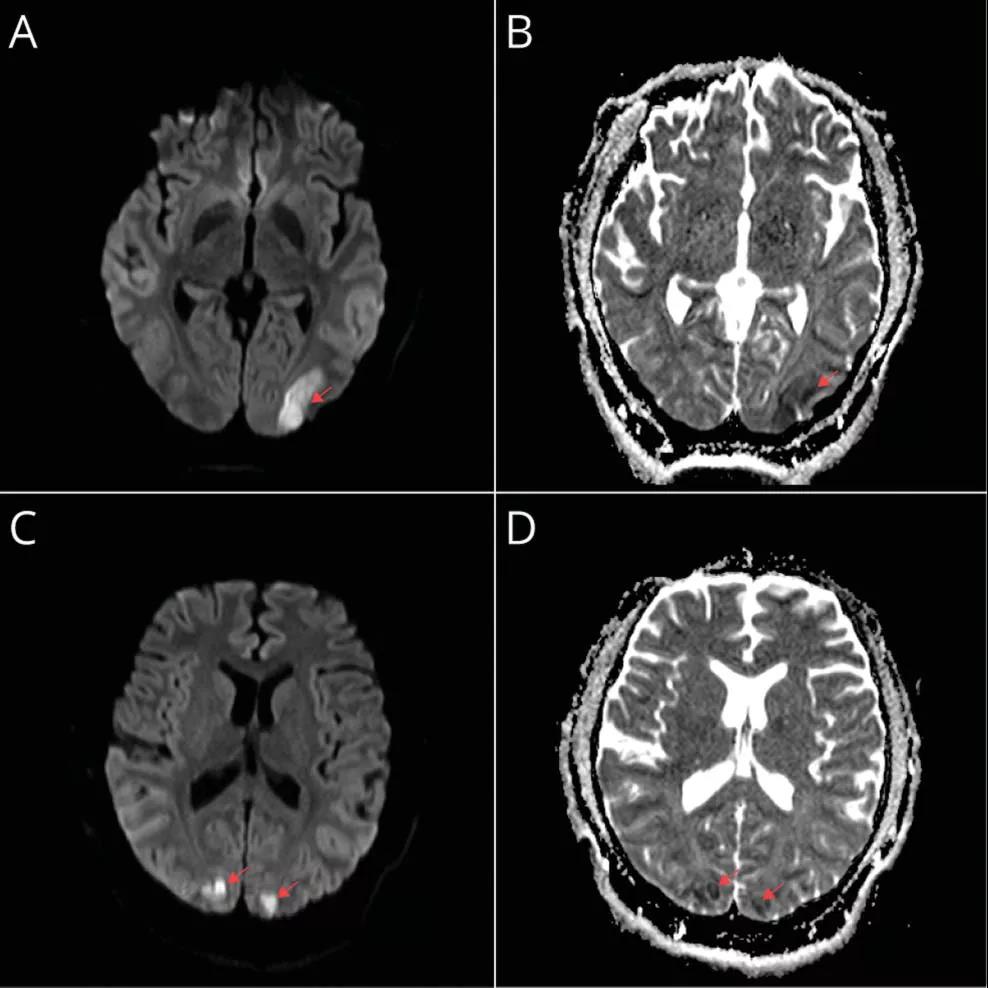
下图2.(A)和(B)为入院时MRI;DWI(A)和ADC(B)序列显示左侧顶枕叶急性梗死。(C)和(D)在头痛和视力丧失急性恶化时完成,DWI(C)和ADC(D)序列显示新发缺血性梗死:
神经源性膀胱可以触发自主神经反射障碍(ered autonomic dysreflexia,AD),从而引发RCV。
T6脊髓水平以上的损伤可消除脊髓上调制(eliminates supraspinal modulation),并可导致AD,即过度的交感反射,从而引起的发作性高血压和心动过缓(译者注:为什么心动过缓,不是心动过速)。放置导尿管(suprapubic catheter placement)后,发作停止,TCD速度正常,视力恢复。
原始出处:
Christina M. Lineback, Eric W. Moffet, Minjee Kim. Teaching NeuroImage: Neurovascular Consequences of Autonomic Dysreflexia. Neurology. 2021 Oct 21;10.1212/WNL.0000000000013011. doi: 10.1212/WNL.0000000000013011. Online ahead of print.
本网站所有内容来源注明为“williamhill asia 医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于williamhill asia 医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“williamhill asia 医学”。其它来源的文章系转载文章,或“williamhill asia 号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与williamhill asia 联系,williamhill asia 将立即进行删除处理。
在此留言







#Neurol#
83
#可逆性脑血管收缩综合征#
66
#血管收缩#
66
#综合征#
58
#可逆性#
77