
Arthritis Rheumatol :利妥昔单抗+环磷酰胺+贝利木单抗治疗狼疮性肾炎的II期随机试验
2021-09-24 从医路漫漫 MedSci原创
评估利妥昔单抗联合贝利木单抗治疗难治性狼疮肾炎(LN)的安全性、作用机制和初步疗效。

目的:评估利妥昔单抗联合贝利木单抗治疗难治性狼疮肾炎(LN)的安全性、作用机制和初步疗效。
方法。在一项多中心、随机、开放标签的临床试验中,43例复发或难治性LN患者接受利妥昔单抗、环磷酰胺(CYC)和糖皮质激素治疗,随后每周输注贝利木单抗直到第48周(RCB组),或使用利妥昔单抗和CYC但不输注贝利木单抗(RC组)。患者随访至第96周。采用流式细胞术分析患者外周血中总B细胞和自体B细胞亚群的百分比。
结果:贝利木单抗治疗并没有增加难治性LN患者不良事件的发生率。在第48周,接受贝利木单抗治疗的21例患者中有11例(52%)发生了完全或部分肾脏反应,相比之下,RC组未接受贝利木单抗治疗的22例患者中有9例(41%)发生了完全或部分肾脏反应(P = 0.452)。LN缺乏改善或恶化是治疗失败的主要原因。两组均出现B细胞衰竭,但贝利木单抗组B细胞百分比仍较低(第60周B细胞几何平均数量,RCB组53细胞/μl, RC组11细胞/μl;P = 0.0012)。两组中总和自反应性过渡B细胞的百分比从基线到48周均有所增加。然而,与没有贝利木单抗的RC组相比,贝利木单抗组中总和自体反应的初代B细胞百分比从基线到第48周下降(P = 0.0349),这一发现与初代B细胞成熟受损和自体反应B细胞截短增强相一致。
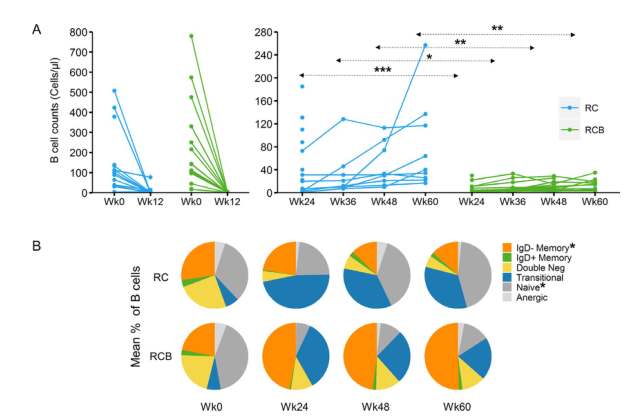
图1 狼疮性肾炎患者外周血单个核细胞(PBMC)中B细胞总数和RC与RCB治疗后B细胞亚群的相对数目。治疗前、治疗后12周(左)和RC或RCB治疗后24-60周重建期间,外周血中A、B细胞计数(左)和RCB治疗后24-60周(右)外周血中A、B细胞计数。每个数据点代表单个患者的外周血液中的临床实验室检测所确定的CD19+B细胞计数。*=P<0.001;**=P<0.01;*=P<0.001。多重比较采用Tukey-Kramer事后调整。B,通过对冻存PBMC的流式细胞术分析,在每个治疗组的每个时间点,每个治疗组中每个B细胞亚群在总B细胞中的平均频率,包括在0周和24周分析的按方案样本和在48周和60周分析的按方案样本。对每个评估时间点的B细胞亚群数据进行分析,找出>50个细胞的亚群。*=治疗组间比较P<0.01。
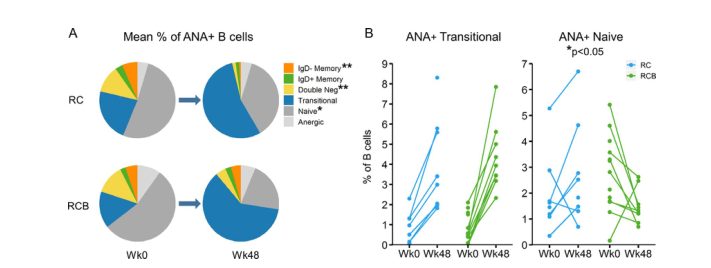
图2 48周时,在符合方案的人群中,RC与RCB治疗后自身反应性抗核抗体阳性(ANA+)B细胞亚群的重建。A,治疗前和治疗后48周各组ANA+B细胞中B细胞亚群的平均数目。*=P<0.05;**=48周各组间P<0.01。B细胞、ANA+过渡性B细胞和ANA+幼稚B细胞占治疗前和治疗48周时外周血中总B细胞的百分比。每个数据点代表单个患者在每个时间点ANA+移行B细胞(左)或ANA+幼稚B细胞(右)的相对频率,用Fisher‘s精确检验确定P值。
结论:在难治性LN患者中,将贝利木单抗增加到利妥昔单抗和CYC治疗方案中是安全的。这种方案减少了B细胞重建过程中过渡到幼稚B细胞的成熟,并增强了自体反应B细胞的阴性选择。在狼疮性肾炎患者中,利妥昔单抗和环磷酰胺联合贝利木单抗与单独使用B细胞去除治疗策略相比,临床疗效没有改善。
原文出处:
Atisha-Fregoso Y,Malkiel S,Harris KM,et al,Phase II Randomized Trial of Rituximab Plus Cyclophosphamide Followed by Belimumab for the Treatment of Lupus Nephritis.Arthritis Rheumatol 2021 01;73(1)
本网站所有内容来源注明为“williamhill asia 医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于williamhill asia 医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“williamhill asia 医学”。其它来源的文章系转载文章,或“williamhill asia 号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与williamhill asia 联系,williamhill asia 将立即进行删除处理。
在此留言







#利妥昔#
0
#Arthritis#
80
好文
66
好文章
108
#环磷酰胺#
94
#ART#
61
#狼疮#
60
#随机试验#
0
#肾炎#
62