

一,疾病概述
抗磷脂综合征(Anti- phospholipid syndrome,APS)是一种非炎症性自身免疫病,临床上以动静脉血栓形成、习惯性流产和血小板减少等症状为表现,血清中存在抗磷脂抗体(aPL),上述症状可以单独或多个共同存在。
APS可分为原发性抗磷脂综合征(PAPS)和继发性抗磷脂综合征(SAPS),SAPS多见于系统性红斑狼疮或类风湿关节炎等自身免疫病。此外,还有一种少见的恶性抗脂综合征,表现为短期内进行性广泛血栓形成,造成多器官功能衰竭甚至死亡。
PAPS的病因目前尚不明确,可能与遗传感染等因素有关。多见于年轻人,男女发病比率为1:9,女性中位年龄为30岁。
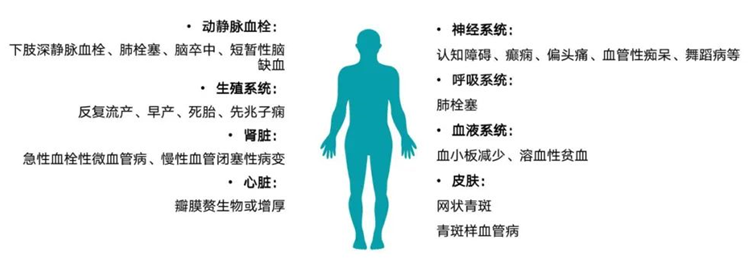
二,临床表现
APS的主要表现是血栓事件、习惯性流产。但也有会累及其他多个脏器。
三,诊断与鉴别诊断
1、诊断:原发性APS的诊断主要依靠临床表现和实验室检查,还必须排除其他自身免疫病和感染、肿瘤疾病引起的血栓。至今国际上无统一的诊断标准。
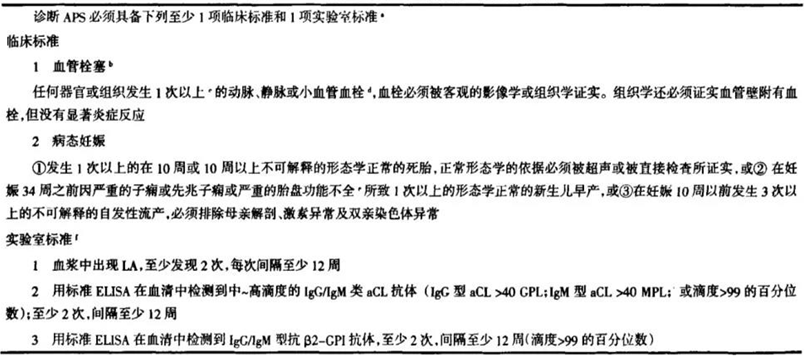
表1 2006年悉尼国际APS会议修订的分类标准
2、鉴别诊断:单从临床表现或实验室检查很难确诊原发性APS。一个有中高滴度aCL或LA阳性的患者,并有以下情况应考虑APS可能:
①无法解释的动脉或静脉血栓
②发生在不常见部位的血栓(如肾或肾上腺)
③年轻人发生的血栓
④反复发生的血栓
⑤反复发作的血小板减少
⑥发生在妊娠中晚期的流产
Ø 静脉血栓需与蛋白C、蛋白S和抗凝血酶Ⅲ缺陷症、血栓性血小板减少性紫廠、纤溶异常、肾病综合征、阵发性夜间血红蛋白尿、白塞病及与口服避孕药相关的血栓等疾病相鉴别。
Ø 动脉血栓需与高脂血症、糖尿病血管病变、血栓闭塞性脉管炎、血管炎、高血压等疾病相鉴别。
四,治疗
1、一般治疗
Ø 对原发性APS的治疗主要是对症处理、防止血栓和流产再发生,一般不需用激素或免疫抑制剂治疗。
Ø 对于继发性APS,如继发于SLE或伴有严重血小板减少(<50×109/L)或溶血性盆血等特殊情况,可以使用激素或免疫抑制剂治疗。
Ø 抗疑治疗主要应用于aPL阳性伴有血栓患者,或体阳性又有反复流产史的孕妇。
Ø 对无症状的抗体阳性患者不宜进行抗疑治疗。

注:ASA 阿司匹林;INR 国际标准化比率
表2 APS伴中高滴度aPL患者的治疗方案
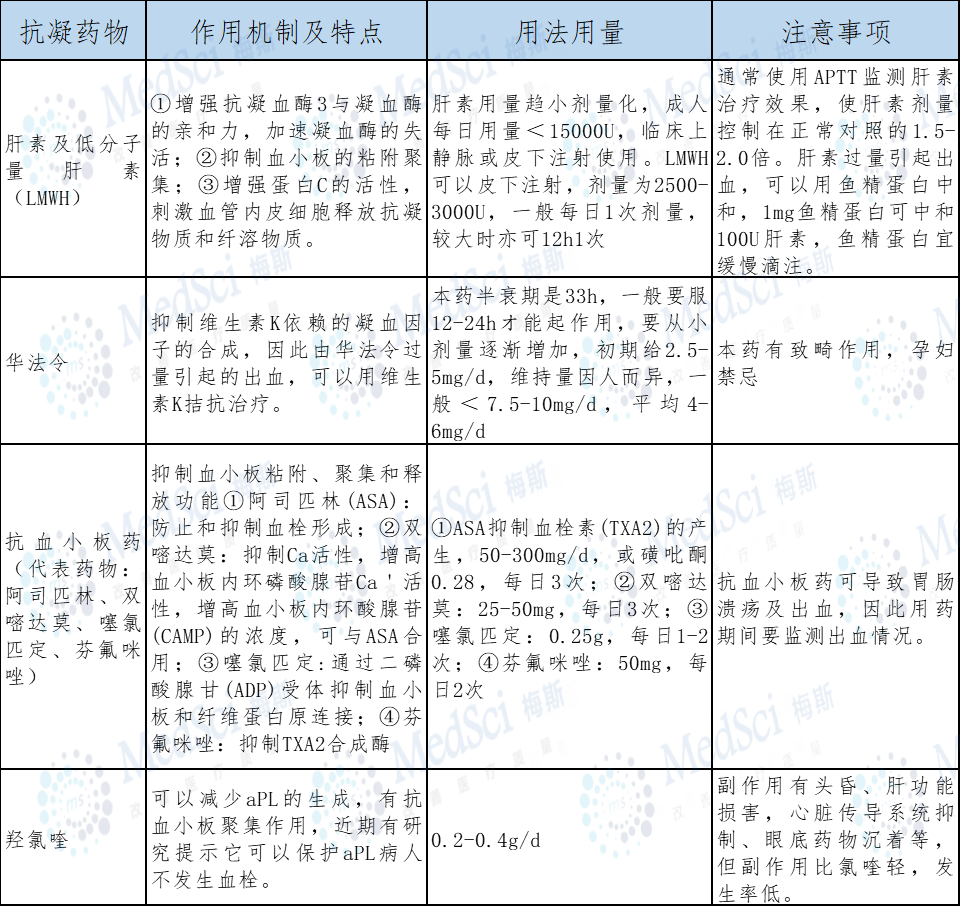
表3 常用的抗凝药物
2、急性期治疗
急性期血栓可行取栓术,静脉血栓在72h内手术,动脉血栓在8-12h内行取栓术或血管旁路术。有手术禁忌证者,可以溶栓,国内常用的药物有尿激酶、链激酶,溶栓后用肝素或华法令抗凝治疗。但是临床经验提示溶栓药物对APS无效,因为很快会再次发生再栓塞。
3、慢性期治疗
在慢性期以口服抗凝治疗为主,长期抗凝治疗会降低血栓的复发率,但亦会增加出血风险,应特别注意。抗凝治疗应监测INR,对动脉血栓应控制在2.5-3.0,静脉血栓则宜在2.0-3.0,经良好抗凝治疗仍发生血栓的患者,可试用羟氯喹。
4、妊娠期治疗:
APS孕妇应分情况处理
Ø 既往无流产史,或妊前10周发生的流产,通常以小剂量ASA治疗
Ø 既往有妊娠10周发生的流产病史,在确认妊娠后,皮下注射肝素5000,每日2次,直至分娩前停用
Ø 既往有血栓史,在妊娠前就开始用肝素或低分子肝素抗凝治疗,在妊娠期不用华法令
Ø 产后治疗,由于产后前3个月发生血栓的风险极大,故产后应该继续抗凝治疗6-12周,如果可能,在产后2-3周内可以把肝素改用为华法令。
5、血小板计数减少的治疗
Ø 对血小板计数>50×109/L的轻度血小板计数减少而不合并血栓的病人,可以观察
Ø 对有血栓而血小板计数>100×109/L病人要谨慎抗凝治疗
Ø 血小板计数>50×109/L禁止抗凝,可以用泼尼松1-2mg・kg-1・d-1,大剂量静脉丙种球蛋白注射,400mg/kg,待血小板上升后抗凝治疗。
6、恶性抗磷脂抗体综合征
本综合征常是骤然起病,一般主张抗凝并同时使用较大量激素,必要时联合使用血浆置换和静脉注射免疫球蛋白。
本网站所有内容来源注明为“williamhill asia 医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于williamhill asia 医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“williamhill asia 医学”。其它来源的文章系转载文章,或“williamhill asia 号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与williamhill asia 联系,williamhill asia 将立即进行删除处理。
在此留言









学习了
69
学习了
69
学习啦
75
#综合征#
61
学习了
86