AACR 2022:围手术期帕博利珠单抗联合卡培他滨和奥沙利铂及辅助帕博利珠单抗治疗可切除胃和胃食管结合部(GC/GEJ)腺癌的II期试验
2022-04-11 网络 网络

2019年ASCO会议上,KEYNOTE-062研究公布了最新结果,纳入763例局部晚期、HER2阴性、PD-L1 CPS≥1的不可切除或转移性GC/GEJC患者,在PD-L1 CPS≥1
2019年ASCO会议上,KEYNOTE-062研究公布了最新结果,纳入763例局部晚期、HER2阴性、PD-L1 CPS≥1的不可切除或转移性GC/GEJC患者,在PD-L1 CPS≥1的患者中,帕博利珠单抗单药的OS非劣效于化疗组;在PD-L1 CPS≥10的患者中,虽然帕博利珠单抗的OS相比于化疗取得了有临床意义的OS改善,但其联合化疗对比单纯化疗用于晚期GC/GEJC一线治疗,并未观察到无进展生存(PFS)或OS的改善。但是,针对围手术期的可切除胃和胃食管结合部(GC/GEJ)腺癌的研究结果,此前一直未知。有关晚期的研究结果见:盘点晚期胃癌免疫一线治疗新进展@MedSci
围手术期治疗是局部晚期(LA)GC/GEJ腺癌治疗的标准治疗。尽管放化疗和手术切除序贯免疫检查点抑制剂(ICB),显著提高了食管癌的无病生存率(DFS),但尚不清楚ICB联合化疗在LA GC/GEJ中的有效性。
这是一项多中心、单臂、II期临床试验,对可切除GC/GEJ腺癌患者进行帕博利珠单抗200mg/每3周联合卡培他滨625 mg/㎡每日两次和奥沙利铂130 mg/㎡每3周(CAPOX)治疗。ECOG PS为0-1的受试者在术前和术后分别接受了3个周期的CAPOX联合帕博利珠单抗治疗,而且,在手术前还会另外增加1个周期的帕博利珠单抗,并在辅助化免治疗后接受12个月的帕博利珠单抗维持治疗。主要终点是病理完全缓解(pCR)率。该研究具有80%的效能检测出pCR率从3%增加到15%,单侧α为0.05。次要终点包括总缓解率、DFS和总生存率(OS)。本研究在ClinicalTrials.gov注册(NCT02918162)。
在2017年2月10日至2021年6月17日期间,纳入了36例患者,其中34例(21例胃癌,13例GEJ)可进行疗效评估。中位年龄为65岁,17例(50%)患者的ECOG PS为1。总计29例(85%)患者接受了切除手术。7名患者达到pCR(20.6%的可评估患者和24.1%的切除患者)。另有6例(17.6%)患者接近完全缓解(CR),8例(23.5%)在病理审查中显示出显著的治疗效果。1例患者被认为不适合手术,2例患者在手术前死亡,2例患者在手术中发现有转移。
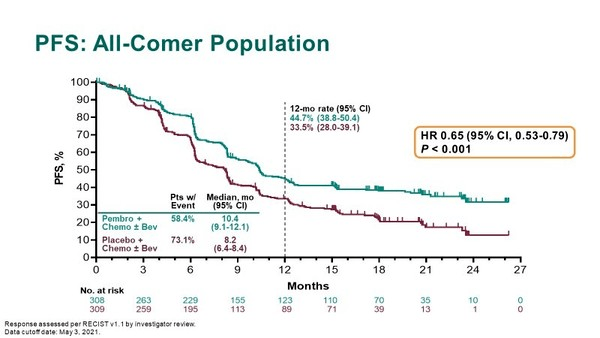
数据截止时,中位随访时间为19个月。在接受切除的患者中,4例(13.7%)出现疾病复发,5例(17.2%)死亡。1年和2年生存率分别为91%(0.82-1.0)和80%(0.64-0.99)。中位DFS和OS未达到。在接受治疗的35例患者中,18例(51%)患者报告了大于等于3级的治疗相关不良事件(AE)。在10例(29%)患者中报告了大于等于3级的免疫相关AE。发生了3例5级AE,2例可能与治疗相关(胃出血和胃穿孔),1例与治疗无关(心脏骤停)。
综上,在LA GC/GEJ腺癌中,CAPOX和帕博丽珠单抗的联合治疗使pCR率达到20.6%。该组合的耐受性良好,85.3%的患者接受了手术切除。这项试验达到了主要终点,支持进一步研究这种方案,作为不太可能容忍三联化疗的患者的替代方案。
本网站所有内容来源注明为“williamhill asia 医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于williamhill asia 医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“williamhill asia 医学”。其它来源的文章系转载文章,或“williamhill asia 号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与williamhill asia 联系,williamhill asia 将立即进行删除处理。
在此留言








#手术期#
61
#铂#
84
#帕博利珠单抗#
86
#博利珠单抗#与#食管癌#
108
#帕博利珠#
52
#胃食管#
54
#II期试验#
70
#卡培他滨#
64
#ACR#
63
#食管#
47