Eur Urol Oncol:雄激素阻断疗法与多西他赛联用治疗高风险生化复发前列腺癌
2021-06-06 AlexYang MedSci原创

局部前列腺癌患者根治性前列腺切除术后的生化复发(BCR)率为15-30%,其中三分之一的患者在常规影像学上有可见病变。尽管放射治疗(RT)加上或不加上雄激素阻断治疗(ADT)可以治愈一部分患者,但治疗
局部前列腺癌患者根治性前列腺切除术后的生化复发(BCR)率为15-30%,其中三分之一的患者在常规影像学上有可见病变。尽管放射治疗(RT)加上或不加上雄激素阻断治疗(ADT)可以治愈一部分患者,但治疗方法仍不确定。预后因素(包括高Gleason评分、从手术到前列腺特异性抗原(PSA)再次恶化的时间短,以及PSA翻倍时间(PSADT)短)可以确定哪些男性有全身扩散和疾病死亡的高风险。

对于前列腺切除术后的高风险生化复发(BCR)患者,目前尚无标准的治疗方法。近期,有研究人员评估了在雄激素阻断疗法(ADT)中加入多西他赛是否能改善高风险BCR患者的无进展生存期(PFS)。
TAX3503是一项多中心的3期试验,对高风险BCR患者随机进行18个月的ADT治疗(加或不加多西他赛)(75mg/m2 q3w,10个周期)。入选标准包括单纯前列腺切除术后或术后放疗后前列腺特异性抗原(PSA)≥1.0ng/ml,PSA翻倍时间≤9个月,以及计算机断层扫描和骨扫描未发现转移。研究的主要终点是睾酮恢复到非去势水平(睾酮>50ng/dl)后的PFS。次要终点包括睾酮恢复的时间、总生存期(OS)、生活质量和安全性。
2007年9月至2011年5月期间,共有413名患者分配到ADT±多西他赛治疗。2012年,在完成应计和治疗后,赞助者撤回了对他们研究的支持。2013年,研究人员建立了一个登记册以确保主要终点。最后分析的数据来子原始试验和注册中心。在中位数为33.6个月的随访中,260名患者的睾丸激素恢复,且各组之间产生的情况相似。ADT加多西他赛对睾酮恢复人群的PFS(中位数26.2个月 vs 24.7个月)(218名,HR 0.80,95%CI 0.61-1.04)和意向治疗人群的OS(中位数未达到,HR 0.51,95%CI 0.23-1.10)有非临床意义的改善。在ADT加多西他赛组,≥3级的不良事件发生得更频繁(48.0% vs 10.8%)。
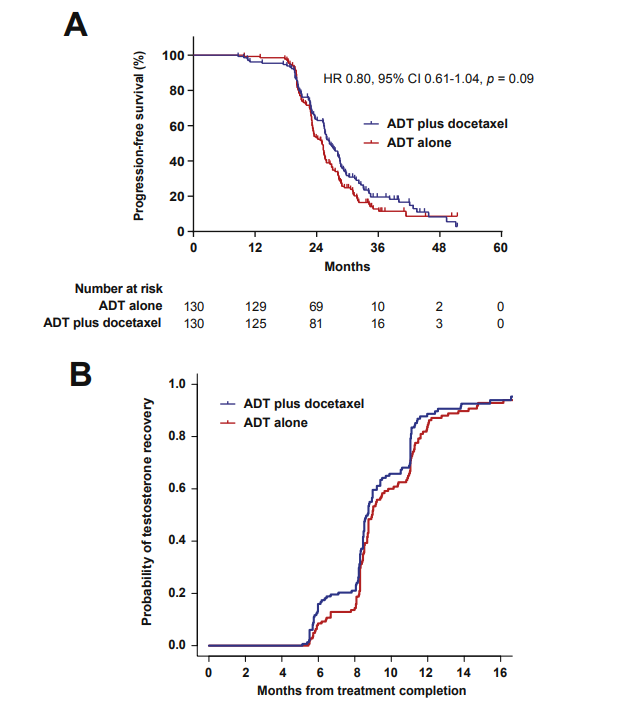
睾酮恢复人群中的结局
综上所述,TAX3503没有证明在高风险BCR患者的ADT治疗中加入多西他赛具有显著的益处。另外,睾丸激素的恢复不受多西紫杉醇加入ADT治疗的影响。
原始出处:
Michael J Morris, Jose Mauricio Mota, Kristine Lacuna et al. Phase 3 Randomized Controlled Trial of Androgen Deprivation Therapy with or Without Docetaxel in High-risk Biochemically Recurrent Prostate Cancer After Surgery (TAX3503). Eur Urol Oncol. May 2021
本网站所有内容来源注明为“williamhill asia 医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于williamhill asia 医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“williamhill asia 医学”。其它来源的文章系转载文章,或“williamhill asia 号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与williamhill asia 联系,williamhill asia 将立即进行删除处理。
在此留言









#阻断疗法#
67
#联用治疗#
64
#Oncol#
59
#高风险#
66
#阻断#
60
#雄激素阻断#
60
#雄激素阻断疗法#
59
#生化复发#
55
谢谢williamhill asia 分享这么多精彩信息
75
前列腺癌相关研究,学习了,谢谢williamhill asia
72